Building modern EMR functionality in 2026 involves a distinct complexity profile from what it was five years ago. The FHIR-first assumption changes what teams should invest in.
1. HL7v2 ingestion is still primary data source. Despite the FHIR mandate, most upstream clinical data arrives as HL7v2 messages. Investment: HL7v2-to-FHIR converter with edge-case handling for OBX repeats, ADT^A08 update semantics, and PV1-3 location resolution.
2. Terminology binding governance. US Core mandates specific ValueSets. Investment: terminology server infrastructure with quarterly SNOMED updates.
3. SMART on FHIR launch stack. SMART launch is the third-party integration surface. Investment: OAuth server supporting v2 scopes, launch context management, refresh tokens for background apps.
4. Bulk data as an operational surface. Bulk Data IG is table-stakes. Investment: $export infrastructure, output storage, manifest hosting, expiry cleanup.
5. Auth boundary. Multi-tenant EMR requires per-tenant auth isolation. Investment: tenant-scoped tokens, cross-tenant read prevention.
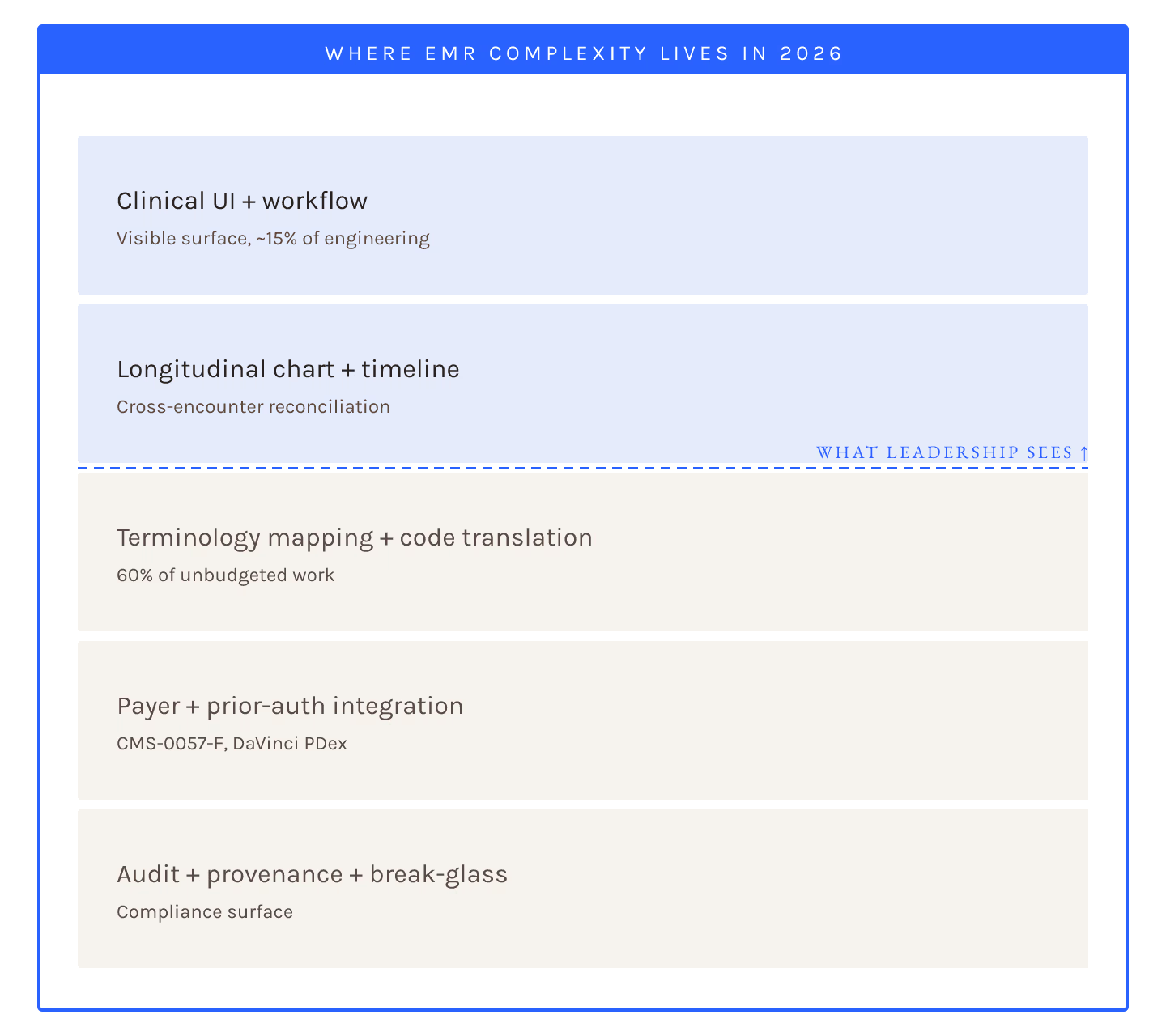
Investment breakdown
| Subsystem | Typical spend | Deferrable? |
|---|---|---|
| HL7v2 converter | ~20% | No, upstream data depends |
| Terminology server | ~15% | No, CMS-0057 requires |
| SMART launch | ~15% | No, third-party ecosystem |
| Bulk data | ~15% | Somewhat, but coming due |
| Auth boundary | ~15% | No, security |
| Application UI | ~20% | Later phases |
EMR development in 2026 is 60-70% infrastructure engineering. Product features layer on top of the FHIR primitives; the primitives take the majority of the work.